








Benefits

Calcium & Fluoride Release
Continuous calcium and fluoride release.

Alkaline Ph
Calcium-silicate fillers provide both calcium release and alkalinity.

Contains MDP
Contains the adhesion promoting monomer MDP.

High Degree of Conversion
A high degree of conversion ensures enhanced physical properties.
High Compressive Strength
Absorbs shock and stress from occlusal forces without fracturing.

Self-Adhesive Cement
Self-adhesive! No bonding agents required.

Radiopaque
Radiopaque for easy detection on radiographs.

Dual-Cured
Dual-cured material.

Auto-Mix
Auto-mix, dual-syringe provides a consistent mix for immediate delivery.

Low Film Thickness
Low film thickness ensures the restoration is completely seated.

Strong Bond to Zirconia
Enhances the bond strength to Zirconia.

Easy Clean Up
Formulated to allow for quick and easy removal of excess cement.
Description
Self-Adhesive Resin Cement
TheraCem is a dual-cured, calcium and fluoride-releasing, self-adhesive resin cement indicated for luting crowns, bridges, inlays, onlays and posts (prefabricated metal/non-metal/fiber posts).
TheraCem delivers a strong bond to Zirconia and most substrates, along with easy clean-up and high radiopacity, offering the clinician a reliable and durable cementation of indirect restorations.
TheraCem 8g auto-mix dual-syringe can provide approximately 14 restorations.
Unique Benefits:
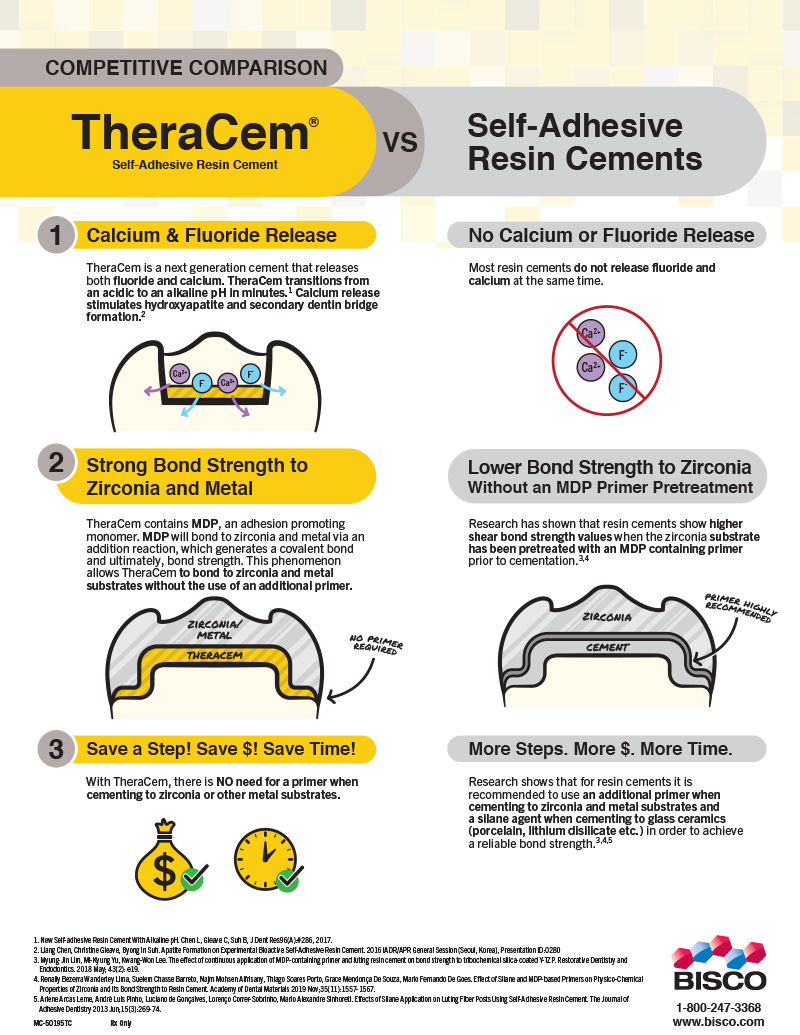
- Provides a continuous calcium and fluoride release*
- Transitions from an acidic to alkaline pH in minutes*
- Contains MDP, allowing for a strong bond to Zirconia, Metal, and Alumina substrates without the use of an additional primer
- Specially formulated to allow for quick and easy clean-up
- A high degree of conversion ensures a higher physical strength
- Easy to identify on radiographs for quick and effective diagnosis
- Easy auto-mix, dual-syringe provides a consistent mix for immediate delivery
Clinical Significance:
- Delivers a strong bond to Zirconia and most substrates with no priming or etching required
Pro Tip:
- Tack-cure for 2-3 seconds to facilitate excess cement removal
In the box
- 1 Dual-Syringe TheraCem (8g)
- 15 Mixing Tips and Intraoral Tips
- Instructions
Benefits
Calcium & Fluoride Release
Continuous calcium and fluoride release.
Alkaline Ph
Calcium-silicate fillers provide both calcium release and alkalinity.
Contains MDP
Contains the adhesion promoting monomer MDP.
High Degree of Conversion
A high degree of conversion ensures enhanced physical properties.
High Compressive Strength
Absorbs shock and stress from occlusal forces without fracturing.
Self-Adhesive Cement
Self-adhesive! No bonding agents required.
Radiopaque
Radiopaque for easy detection on radiographs.
Dual-Cured
Dual-cured material.
Auto-Mix
Auto-mix, dual-syringe provides a consistent mix for immediate delivery.
Low Film Thickness
Low film thickness ensures the restoration is completely seated.
Strong Bond to Zirconia
Enhances the bond strength to Zirconia.
Easy Clean Up
Formulated to allow for quick and easy removal of excess cement.
Awards
Dental Advisor Top Innovative Cement
Dental Advisor Preferred Self-Adhesive Cement
DPS Best Product
Dental Advisor Editors Choice
Instructions
Brochure


SDS
TheraCem Base SDS US English
EnglishTheraCem Catalyst SDS US English
EnglishTheraCem Base SDS US French
FrenchTheraCem Base SDS US Portuguese
PortugueseTheraCem Base SDS US Russian
RussianTheraCem Base SDS US Spanish
SpanishTheraCem Catalyst SDS US French
FrenchTheraCem Catalyst SDS US Portuguese
PortugueseTheraCem Catalyst SDS US Russian
RussianTheraCem Catalyst SDS US Spanish
Spanish
All-Bond Universal ®
BISCO’s All-Bond Universal allows you to standardize clinical protocols for effective delivery of adhesion with a single-bottle.
All-Bond Universal ®
BISCO’s All-Bond Universal allows you to standardize clinical protocols for effective delivery of adhesion with a single-bottle.
All-Bond Universal ®
BISCO’s All-Bond Universal allows you to standardize clinical protocols for effective delivery of adhesion with a single-bottle.
All-Bond Universal ®
BISCO’s All-Bond Universal allows you to standardize clinical protocols for effective delivery of adhesion with a single-bottle.
All-Bond Universal ®
BISCO’s All-Bond Universal allows you to standardize clinical protocols for effective delivery of adhesion with a single-bottle.
All-Bond Universal ®
BISCO’s All-Bond Universal allows you to standardize clinical protocols for effective delivery of adhesion with a single-bottle.
All-Bond Universal ®
BISCO’s All-Bond Universal allows you to standardize clinical protocols for effective delivery of adhesion with a single-bottle.
What shade is TheraCem’s “Natural”?
TheraCem’s “Natural” shade is most similar to a “Dentin” shade.
Can TheraCem be used with an additional bonding agent (i.e. All-Bond Universal) for added bond strength?
Although separate adhesive bonding agents can be used with any self-adhesive cement, using additional primers or adhesives with TheraCem may disrupt the Calcium and Fluoride release. If added bond strength is required, BISCO recommends using All-Bond Universal and Duo-Link Universal.
I know TheraCem has MDP, but what happens if you use Z-PRIME Plus & TheraCem?
Applying Z-PRIME Plus to the substrate is not required when cementing with TheraCem. There are neither benefits nor consequences to using them together. Save time, and money and take advantage of TheraCem’s benefits!
With what type of substrates can TheraCem can be used?
TheraCem is compatible with a variety of substrates including zirconia, lithium disilicate (e.max) and feldspathic porcelain.
What is the difference between TheraCem and BisCem?
Both TheraCem and BisCem are self-adhesive cements. However, TheraCem includes the following features as compared to BisCem:
• Fluoride and calcium release
• Higher bonds strengths; especially to Zirconia – Contains MDP
• 18-month shelf life at room temperature (BisCem requires refrigeration)
• Higher radiopacity and can be easily identified on a radiograph
• Easy clean-up and removal of excess cement
• Alkaline pH after bonding
Do I need to use silane on my glass ceramics restorations?
Yes, in order to achieve reliable cementation results, all glass ceramic substrates should be pre-treated with a silane primer such as BISCO’s Porcelain Primer.
